Type of publication:
Poster presentation
Author(s):
*Dr Amy Ingham Farrow; *Dr Emily Thorley
Citation:
Journal of Healthcare Simulation 2024;4(Suppl 1):A67
Abstract:
Introduction:
As an educational modality, simulation “can improve the quality and impact of training provided to doctors now and in the future” [1] but is labour and time intensive due to the small group sizes required to achieve maximum efficacy [2]. Foundation doctors currently undertake two and a half days of multidisciplinary simulation, with scenarios constructively aligned to their curriculum [3]. The need for additional simulation opportunities that are accessible to larger groups of doctors was identified. These sessions would require a more efficient style of delivery to ensure the engagement of all participants, not just those selected to enter the simulation environment. Could the use of multi-modal teaching transform observing learners into active participants to reach a larger audience?
Methods:
The three-part session was designed as an immersive simulation with an integrated interactive prescribing tutorial. This targeted the acute management of a patient with diabetic ketoacidosis and the following twelve hours of their care. The tutorial tasked all attendees (not just those involved in the simulation) with using the Trust protocol to prescribe appropriate treatment at various intervals in response to simulated clinical findings.
Pre- and post-intervention questionnaires explored participants’ views on styles of teaching and examined any changes in clinical confidence and perceptions around the multi-modal teaching style.
Results:
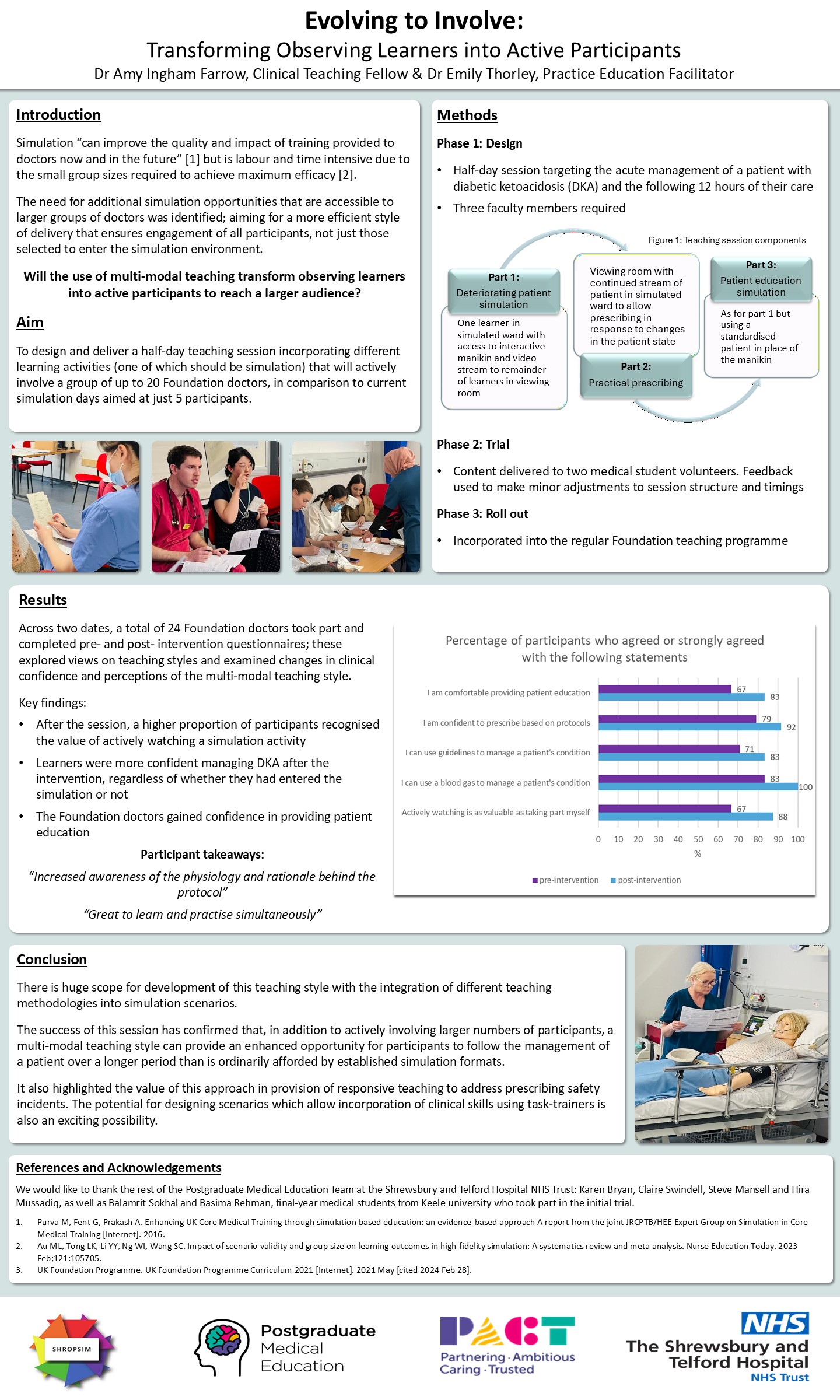
Responses were collected from sixteen Foundation Year 2 doctors who attended the two-hour training afternoon as part of their teaching programme. Data indicated an increase in numbers who agreed or strongly agreed that actively watching scenarios was as valuable as taking part themselves. Additionally, doctors were more confident prescribing treatments based on Trust protocols and were more comfortable using Trust guidelines to manage an unwell patient. Naturally, some challenges arose, with minor changes needed before we repeat this with Foundation Year 1 doctors.
Discussion:
There is huge scope for development of scenarios that integrate different teaching methodologies into simulation-based training. The success of this session has confirmed that, in addition to actively involving larger numbers of participants, a multi-modal teaching style can provide an enhanced opportunity for participants to follow the management of a patient over a longer period than is ordinarily afforded by established simulation formats. It also highlighted the value of this approach in provision of responsive teaching to address prescribing safety incidents. The potential for designing scenarios which allow incorporation of clinical skills using task-trainers is also an exciting possibility.
References:
1. Purva M, Fent G, Prakash A. Enhancing UK Core Medical Training through simulation-based education: an evidence-based approach A report from the joint JRCPTB/HEE Expert Group on Simulation in Core Medical Training [Internet]. 2016. Available from: https://www.jrcptb.org.uk/sites/default/files/HEE_Report_FINAL.pdf
2. Au ML, Tong LK, Li YY, Ng WI, Wang SC. Impact of scenario validity and group size on learning outcomes in high-fidelity simulation: A systematics review and meta-analysis. Nurse Education Today. 2023 Feb;121:105705.
3. UK Foundation Programme. UK Foundation Programme Curriculum 2021 [Internet]. 2021 May [cited 2024 Feb 28]. Available from: https://healtheducationengland.sharepoint.com/sites/UKFPOT/WebDocs/Forms/AllItems.aspx?id=%2Fsites%2FUKFPOT%2FWebDocs%2F4%2E%20Curriculum%2FUKFP%20Curriculum%202021%5FOct22%20update%2Epdf&parent=%2Fsites%2FUKFPOT%2FWebDocs%2F4%2E%20Curriculum&p=true&ga=1
Link to abstract [no password required]
Link to poster [no password required]


{kind=link}