Type of publication:
Journal article
Author(s):
*Savage N.D.S.J. ![]() ; Green J.C.P.; Carley F.
; Green J.C.P.; Carley F.
Citation:
BMJ Case Reports; 2018; vol. 2018
Abstract:
Link to full-text [NHS OpenAthens account required]

Type of publication:
Journal article
Author(s):
*Savage N.D.S.J. ![]() ; Green J.C.P.; Carley F.
; Green J.C.P.; Carley F.
Citation:
BMJ Case Reports; 2018; vol. 2018
Abstract:
Link to full-text [NHS OpenAthens account required]
Type of publication:
Journal article
Author(s):
*Papoutsis, Dimitrios; *Underwood, Martyn ![]() ; *Parry-Smith, William; *Panikkar, Jane
; *Parry-Smith, William; *Panikkar, Jane
Citation:
Archives of Gynecology and Obstetrics; Apr 2018; Vol.297(4):1015-1025
Abstract:
PURPOSE To compare the pregnancy outcomes between women who were treated with cold-coagulation versus large loop excision of the transformation zone (LLETZ) for cervical intraepithelial neoplasia. METHODS This was a retrospective cohort study of women who had a single cervical treatment between 2010 and 2011. We identified those women who had a singleton pregnancy subsequent to their cervical treatment until September 2017. Women with previous cervical treatment, previous miscarriage or preterm delivery were excluded. RESULTSWe identified 86 women with a pregnancy after LLETZ treatment and 75 women after cold coagulation. Those who had LLETZ when compared to cold coagulation miscarried more often in the first trimester (33.7 vs 17.3%; p = 0.01) than in the second trimester. In women with LLETZ this effect of increased early miscarriage was shown to be prolonged and to persist up to 17 months after excision. Women with LLETZ when compared to cold coagulation had higher spontaneous preterm birth rates (8.9 vs 6.7%) even though the difference was non significant, with the earliest spontaneous preterm birth occurring at 32 weeks and 34 weeks, respectively. CONCLUSION We found that women who received LLETZ treatment when compared to cold coagulation had higher spontaneous preterm birth rates in their subsequent pregnancy and miscarried more frequently in the first trimester, and demonstrated an increased early miscarriage risk that persisted for more than a year after excisional treatment.
Altmetrics
Type of publication:
Randomised controlled trial
Author(s):
Ugo Grossi, Natasha Stevens, Eleanor McAlees, *Jon Lacy-Colson, Steven Brown, Anthony Dixon, Gian Luca Di Tanna, S. Mark Scott, Christine Norton, Nadine Marlin, James Mason, Charles H. Knowles, and On behalf of the NIHR CapaCiTY working group
Citation:
Trials; Feb 2018; vol. 19 (no. 1)
Abstract:
Background: Laparoscopic ventral mesh rectopexy (LVMR) is an established treatment for external full thickness rectal prolapse. However, its clinical efficacy in patients with internal prolapse is uncertain due to the lack of high-quality evidence. Methods: An individual level, stepped-wedge randomised trial has been designed to allow observer-blinded data comparisons between patients awaiting LVMR with those who have undergone surgery. Adults with symptomatic internal rectal prolapse, unresponsive to prior conservative management, will be eligible to participate. They will be randomised to three arms with different delays before surgery (0, 12 and 24 weeks). Efficacy outcome data will be collected at equally stepped time points (12, 24, 36 and 48 weeks). The primary objective is to determine clinical efficacy of LVMR compared to controls with reduction in the Patient Assessment of Constipation Quality of Life (PAC-QOL) at 24 weeks serving as the primary outcome. Secondary objectives are to determine: (1) the clinical effectiveness of LVMR to 48 weeks to a maximum of 72 weeks; (2) pre-operative determinants of outcome; (3) relevant health economics for LVMR; (4) qualitative evaluation of patient and health professional experience of LVMR and (5) 30-day morbidity and mortality rates. Discussion: An individual-level, stepped-wedge, randomised trial serves the purpose of providing an untreated comparison for the active treatment group, while at the same time allowing the waiting-listed participants an opportunity to obtain the intervention at a later date. In keeping with the basic ethical tenets of this design, the average waiting time for LVMR (12 weeks) will be shorter than that for routine services (24 weeks).
Altmetrics
Type of publication:
Conference abstract
Author(s):
*Ball W.; *Raza S.S.; *Loy J.; *Riera M.; *Pattar J.; *Adjepong S.; *Rink J.; *Lyons H.; *Price B.
Citation:
Obesity Surgery; Jul 2017; vol. 27 (Supplement 1); p. 335
Abstract:
Introduction: Super Obese patients with body mass index (BMI) > 60KG/M2 pose particular difficulties for primary laparoscopic bariatric surgery. Laparoscopic port access, stapling and suturing become increasingly difficult with higher BMI. Our unit's practice of placing an intragastric balloon for 6 months prior to definitive surgery in patients with BMI > 60KG/M2 aims to make definitive surgery less difficult by reducing weight. Objectives: To quantify weight loss after balloon placement and determine if these patients subsequently underwent definitive bariatric surgery. Methods: Retrospective review of 46 consecutive patients with intragastric balloon placement using SPSS statistical analysis on the results. Results: Median weight loss 14kg (0-42) P<0.0001, median % excess weight loss (%EWL) 15% (-3.3-64.66) P<0.001 and median BMI reduction 5KG/M2 (-1.3-13.9) P<0.001. 29/46 (63%) patients underwent definitive bariatric surgery. 10/46 (22%) patients had minor complications (nausea, vomiting and pain) requiring re-admission, of these 7/10 (70%) had early balloon removal and 6/10 (60%) did not have definitive bariatric surgery. 6/46 patients had second balloon placement median weight loss-6kg (-22-33), median %EWL-4.85% (-21.6-34.96), median BMI reduction-1.3KG/M2 (-8.5-2.5). Conclusion: Results from intragastric balloon placement are encouraging and comparable with a recent metaanalysis. Re-admissions and low %EWL with the first balloon are predictors for early balloon removal and failure to proceed to definitive surgery. Intragastric balloons as a bridge to definitive bariatric surgery are effective and safe. Sequential intragastric balloons are not recommended.
Type of publication:
Journal article
Author(s):
*Quraishi M.K.; *Phan Y.C.; *Asaad W.; *Lynn N.
Citation:
BMJ Case Reports; 2018; vol. 2018
Abstract:
A staghorn calculus is a calculus accommodating the majority of a renal calyx extending into the renal pelvis. A conservative approach to its treatment may lead to high morbidity and mortality rates. Such morbidity usually manifests with renal failure, obstructed upper urinary tractand/or life-Threatening sepsis. Prostatic abscesses have never been associated with staghorn calculi in the literature. We report a case of a 70-year-old man who presented with sepsis, which was found to originate from a complex prostatic abscess. The patient had no history of urinary tract infections or risk factors. The authors believe that the incidentally identified staghorn calculi promoted the growth of Proteus mirabilis which led to the development of the prostatic abscess. The patient underwent a transurethral resection and drainage of the abscess following a failed course of antibiotic therapy. This case also highlights the paucity of guidelines available in treating prostatic abscesses.
Link to full-text [NHS OpenAthens account required]
Type of publication:
Poster presentation
Author(s):
*Smyth, C., *Bowen, J., *Gornall, A.
Citation:
Poster presentation at the ABN – May 2018 Birmingham
Type of publication:
Randomised controlled trial
Author(s):
Iveson TJ, Kerr RS, Saunders MP, Cassidy J, Hollander NH, Tabernero J, Haydon A, Glimelius B, Harkin A, Allan K, McQueen J, Scudder C, Boyd KA, Briggs A, Waterston A, Medley L, Wilson C, Ellis R, Essapen S, Dhadda AS, Harrison M, Falk S, Raouf S, Rees C, Olesen RK, Propper D, Bridgewater J, Azzabi A, Farrugia D, Webb A, Cunningham D, Hickish T, Weaver A, Gollins S, Wasan HS, Paul J. [SaTH was one of the sites this trial took place at]
Citation:
Lancet Oncology 2018 Apr;19(4):562-578
Abstract:
BACKGROUND: 6 months of oxaliplatin-containing chemotherapy is usually given as adjuvant treatment for stage 3 colorectal cancer. We investigated whether 3 months of oxaliplatin-containing chemotherapy would be non-inferior to the usual 6 months of treatment.
METHODS: The SCOT study was an international, randomised, phase 3, non-inferiority trial done at 244 centres. Patients aged 18 years or older with high-risk stage II and stage III colorectal cancer underwent central randomisation with minimisation for centre, choice of regimen, sex, disease site, N stage, T stage, and the starting dose of capecitabine. Patients were assigned (1:1) to receive 3 months or 6 months of adjuvant oxaliplatin-containing chemotherapy. The chemotherapy regimens could consist of CAPOX (capecitabine and oxaliplatin) or FOLFOX (bolus and infused fluorouracil with oxaliplatin). The regimen was selected before randomisation in accordance with choices of the patient and treating physician. The primary study endpoint was disease-free survival and the non-inferiority margin was a hazard ratio of 1·13. The primary analysis was done in the intention-to-treat population and safety was assessed in patients who started study treatment. This trial is registered with ISRCTN, number ISRCTN59757862, and follow-up is continuing.
FINDINGS: 6088 patients underwent randomisation between March 27, 2008, and Nov 29, 2013. The intended treatment was FOLFOX in 1981 patients and CAPOX in 4107 patients. 3044 patients were assigned to 3 month group and 3044 were assigned to 6 month group. Nine patients in the 3 month group and 14 patients in the 6 month group did not consent for their data to be used, leaving 3035 patients in the 3 month group and 3030 patients in the 6 month group for the intention-to-treat analyses. At the cutoff date for analysis, there had been 1482 disease-free survival events, with 740 in the 3 month group and 742 in the 6 month group. 3 year disease-free survival was 76·7% (95% CI 75·1-78·2) for the 3 month group and 77·1% (75·6-78·6) for the 6 month group, giving a hazard ratio of 1·006 (0·909-1·114, test for non-inferiority p=0·012), significantly below the non-inferiority margin. Peripheral neuropathy of grade 2 or worse was more common in the 6 month group (237 [58%] of 409 patients for the subset with safety data) than in the 3 month group (103 [25%] of 420) and was long-lasting and associated with worse quality of life. 1098 serious adverse events were reported (492 reports in the 3 month group and 606 reports in the 6 month group) and 32 treatment-related deaths occurred (16 in each group).
INTERPRETATION: In the whole study population, 3 months of oxaliplatin-containing adjuvant chemotherapy was non-inferior to 6 months of the same therapy for patients with high-risk stage II and stage III colorectal cancer and was associated with reduced toxicity and improved quality of life. Despite the fact the study was underpowered, these data suggest that a shorter duration leads to similar survival outcomes with better quality of life and thus might represent a new standard of care.
FUNDING: Medical Research Council, Swedish Cancer Society, NETSCC, and Cancer Research UK.
Link to full-text [Open access - no password required]
Altmetrics
Type of publication:
Journal article
Author(s):
*Lake, B., Fuller, H.R., *Rastall, S, *Usman, T
Citation:
Indian Journal of Surgery, December 2017
Abstract:
Coping strategies used by women with breast cancer are vital for adjustment to their disease. Whilst it is clear that factors such as age at diagnosis, social support and ethnicity can influence coping mechanisms, there is currently no information about whether breast reconstruction changes mechanisms of coping for such patients. The aims of this study, therefore, were to determine how women who have had immediate breast reconstruction and mastectomy cope, compared to those who have mastectomy alone, and whether there are differences in coping mechanisms due to breast reconstruction surgery. This was a retrospective cohort study, using a standardised questionnaire called the Brief Cope Scale. Inclusion criteria was the following: all women who had immediate breast reconstruction and mastectomy in Shropshire from 2003 to 2014 for ductal carcinoma in situ or node-negative invasive breast cancer. Each patient was matched for year of diagnosis, adjuvant therapy and age to one woman who had mastectomy alone. Two hundred thirty-four questionnaires were sent with a 58% response rate. Significantly more patients from the reconstruction cohort coped by active coping (T value 1.66, P value 0.04) compared to those in the mastectomy alone cohort. In contrast, significantly more patients in the mastectomy alone cohort coped by active venting compared to the reconstruction cohort (T value 1.71, P value 0.04). This study indicates for the first time that breast reconstruction may alter coping mechanisms in breast cancer survivors. Awareness of these coping mechanisms will enable clinicians to provide appropriate, individualised support.
Type of publication:
Journal article
Author(s):
Pratt H, Andrews C, Panescu D, *Lake B.
Citation:
39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Seogwipo, 2017, pp. 3712-3718.
Abstract:
INTRODUCTION:
A rigorous method for assessing the Ventricular Fibrillation (VF) risk of a Random Complex Waveform (RCW) has not been previously available. Real-life hazardous events motivated us to develop such method. An RCW is observable and recordable. It consists of multiple different components randomly added one to the other. Assessment for VF risk exists for non-random waveforms, particularly VF thresholds for 50/60 Hz alternating currents, but not for RCWs.
METHODS:
We developed a method which considers exposure to a segment of an RCW. It transforms complex segment exposure to values which can be compared with AC root-mean-square (rms) magnitude/duration curves, for determination of VF risk. Human contact could occur for any given time duration within the segment. The current of most risk is the greatest found for all possible instances of that duration. This is termed the "Probable Current" (PC) for that duration. All possible exposure durations in the waveform segment are considered, giving a set of PCs, thus allowing the plotting of a PC curve. The PC set is compared with a criterion for VF risk, termed the Justified Current (JC) curve.
RESULTS:
The theory is presented. Demonstrations and examples are given. Code is shown for generating the PC curve.
CONCLUSION:
VF risk can be found for an RCW using the rigorous algorithm presented.
SIGNIFICANCE:
The VF for RCWs has not been considered previously. A rigorous statement of a method for VF risk assessment allows extension from regular waveforms to RCWs.
Type of publication:
Poster presentation
Author(s):
*Zuydam AC, Rogers SN, Grayson, *McLaughlin K, *Probert, Voyce C
Citation:
British Association of Health and Neck Oncologists, BAHNO Annual Scientific Meeting, Royal College of Physicians, London, Friday 12th May 2017
Abstract:
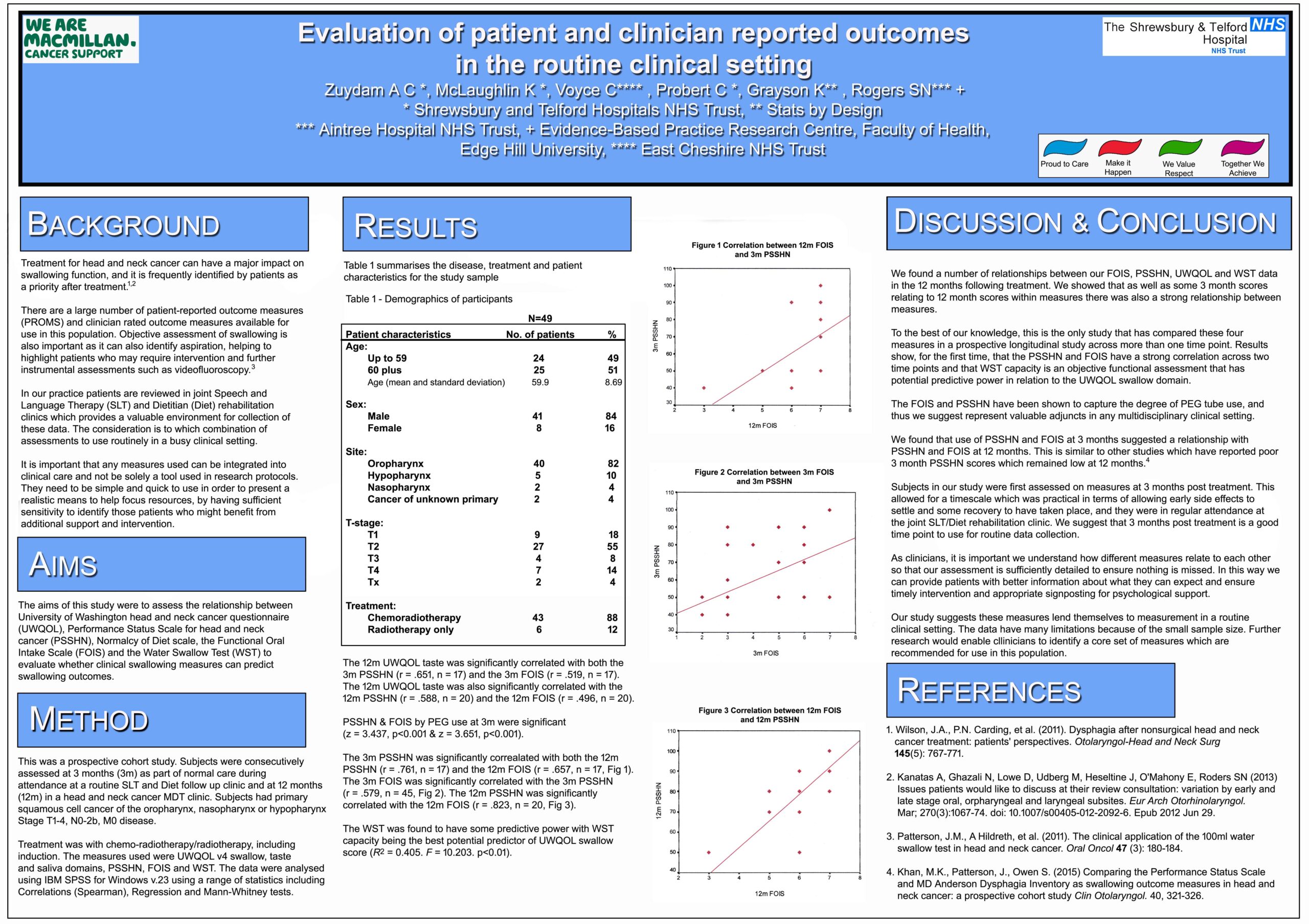
Treatment for head and neck cancer can have an impact on both swallowing function ,and quality of life. It is important that any measures used have sufficient sensitivity to highlight issues .The aims of this study were to assess the relationship between swallowing assessments and to evaluate whether clinical swallowing measures can predict swallowing outcomes.
Methods
This was a prospective cohort study. Subjects had Primary Squamous cell cancer of the oropharynx, nasopharynx or hypopharynx Stage T1‐4, N0‐ 2b, M0 disease. Treatment was with Chemo‐radiotherapy/ radiotherapy ,including induction.The measures used were University of Washington Quality of Life Questionnaire , Performance Status Scale Head and Neck Cancer ( PSSHN) Functional Oral Intake Scale( FOIS ) and the Water Swallow Test ( WST).
Results
Data were collected on 38 patients. The 3m PSSHN was significantly correlated with both the 12m PSSHN (r = .761) and the 12m FOIS (r = .657 ).The 3m FOIS was correlated with the 3m PSSHN (r = .662 ).The 12m PSSHN was significantly correlated with the 12m FOIS (r = .823). The WST was also found to potentially have some predictive power.
Conclusions
A number of measures were found to have clinical significance, and could be valuable to collect in a clinic setting.. Identification of relevant issues early on can enable clinicians to provide patients with information about what they can expect ,and ensure intervention is timely.
Link to poster [no password required]
![]()
Shrewsbury and Telford Hospital NHS Trust has an active Research and Innovation Department.
Find out more by visiting either the R&I Intranet pages (only available on a Trust PC) or the R&I pages on the SaTH website.

Shrewsbury and Telford Hospital NHS Trust has an active Improvement Hub.
Find out more by visiting either the Improvement Hub Intranet pages (only available on a Trust PC) or the Improvement Hub page on the SaTH website.
{kind=link}